Learn how shockwave therapy for Morton’s Neuroma may reduce nerve pain and help avoid surgery. Evidence-based, non-invasive care at Unpain Clinic.
KEY TAKEAWAYS
- Morton's neuroma is an irritated nerve in the ball of your foot. The classic feeling is a sharp, burning, or pebble-like pain between your third and fourth toes.
- Rest, padding, orthotics, and cortisone injections can settle a flare, but they often do not fix the underlying nerve irritation, which is why the pain keeps coming back.
- Shockwave therapy is one of the few non-surgical options with published randomized trial evidence for Morton's neuroma. It reduces pain and improves foot function in most people who try it.
- A typical course is three to six weekly sessions. You will usually know within a few visits whether it is working for you.
- At Unpain Clinic in Edmonton, shockwave therapy is part of a layered plan that also looks at your shoes, your gait, and what is happening higher up in the chain.
If you have been told you have Morton's neuroma, you already know how disruptive it is. One minute you are walking, the next there is a sharp, burning jolt between your toes, or that strange sense of a marble or pebble in your shoe that is not actually there. You have probably tried wider shoes, a metatarsal pad, an over-the-counter insole, maybe even a cortisone shot. Some of it helped for a while. Most of it stopped helping. Surgery is the next step a lot of people get pointed toward, but it is not the only one. Shockwave therapy is a non-surgical option with published randomized trial evidence, and for many people in Edmonton, it is the missing piece. Here is what it is, what the research actually says, and how we use it at Unpain Clinic.
WHAT IS MORTON'S NEUROMA, AND WHY DOES IT FEEL LIKE A PEBBLE IN YOUR SHOE?
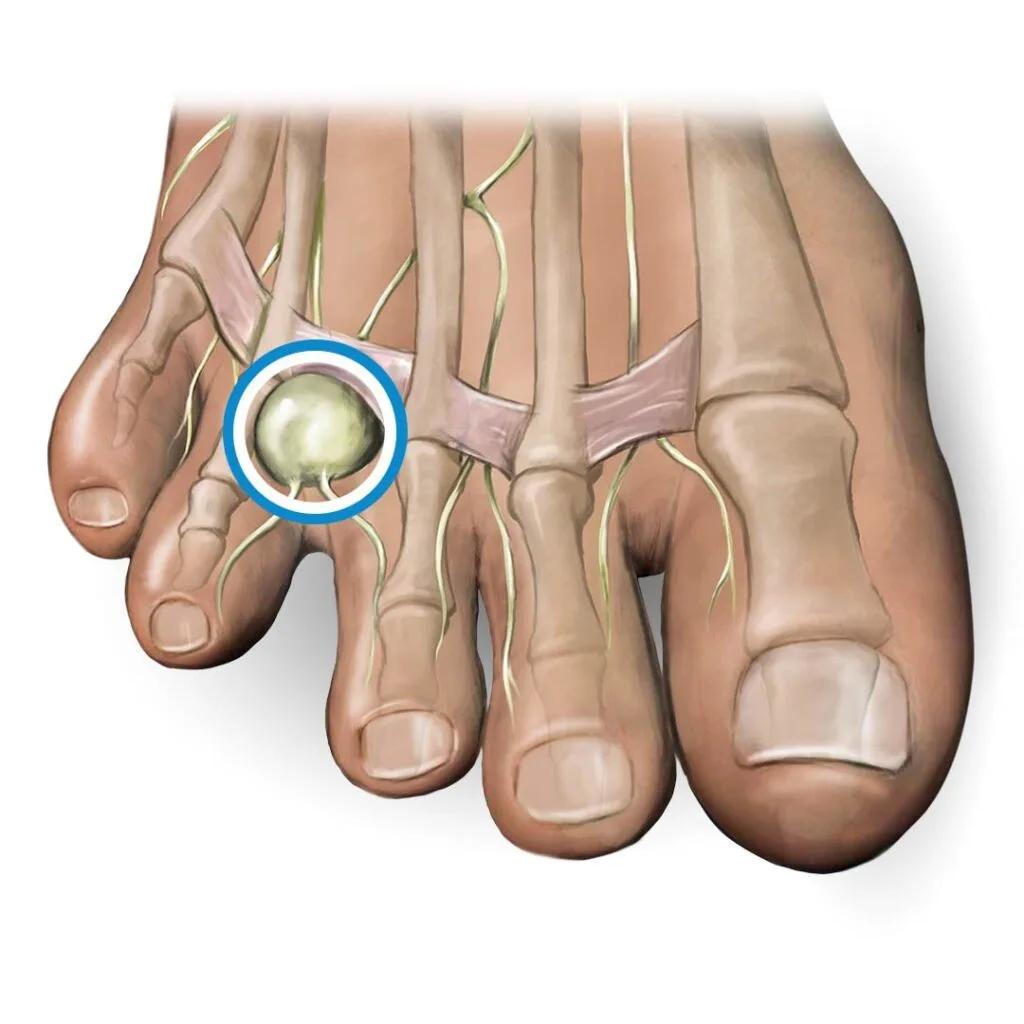
Morton's neuroma is not really a tumour, despite what the name suggests. It is a thickening and irritation of one of the small nerves that runs between your metatarsal bones, almost always between the third and fourth toes. The nerve gets compressed by the bones on either side and by the ligament running across the top of the foot, and over time it thickens, becomes inflamed, and develops the kind of fibrous scarring that keeps it irritated even when you are off your feet.
That is why the pain has its specific feel. The sensation that there is something in your shoe between your toes is the nerve itself getting squeezed when you bear weight on the ball of the foot. The burning or electric quality is the nerve misfiring. The numbness in the toes you sometimes get is the same nerve, just a different way of complaining.
Morton's neuroma is much more common in women than in men, and the usual suspects are repeated forefoot loading and shoes that squeeze the forefoot. Decades of narrow toe boxes, high heels, long days on hard floors, and high-impact activity all add up. Once the nerve is irritated, every step keeps it irritated.

WHY DO ORTHOTICS, CORTISONE, AND REST ONLY HELP FOR SO LONG?
Most people with Morton's neuroma start with the standard advice, and that advice is not wrong. Switch to a wider shoe. Add a metatarsal pad behind the painful spot. Try an orthotic. Take a break from the high-impact stuff. For mild cases caught early, that is sometimes enough.
For everyone else, those steps usually only manage the symptoms. They reduce how much you stress the nerve, but they do not change the nerve itself. The thickened tissue is still thickened. The fibrous scarring is still there. So the moment you put your old shoes back on or go back to your normal activity, the pain comes back.
Cortisone injections often follow. They can give meaningful short-term relief by reducing inflammation around the nerve. But the effect tends to fade over weeks to months, repeated injections come with their own risks (including thinning of the fat pad under the ball of the foot), and they do not address the structural problem either.
That is the gap shockwave therapy fills. It is the only widely available non-surgical option that aims to actually change the tissue around the nerve and calm the nerve itself.
DOES SHOCKWAVE THERAPY ACTUALLY WORK FOR MORTON'S NEUROMA?
The published evidence is small but consistent.
The strongest single piece of evidence is a 2016 randomized, placebo-controlled trial in the Journal of the American Podiatric Medical Association. Patients with Morton's neuroma were randomly assigned to either real shockwave therapy or a sham version. The shockwave group had significantly lower pain scores on a 10-point visual analog scale at one week and four weeks after treatment, and significantly better foot function scores at four weeks. The sham group did not. The neuroma itself did not visibly shrink on ultrasound, but the pain came down and the function went up.
An earlier 2009 randomized, placebo-controlled, double-blind trial in the same journal reported the same pattern at 1, 6, and 12 weeks after treatment. The authors concluded that shockwave therapy is a possible alternative to surgical excision for Morton's neuroma. That language is deliberately careful, and so are we, but it reflects how their data lined up.
A more recent prospective comparison study took it further. Meyer and Moya in 2022 compared focused shockwave therapy head to head with surgical neurectomy in 32 patients. The surgical group had good results in about 93 percent of cases. The shockwave group had good results in about 71 percent. Surgery wins on raw effectiveness, but 71 percent good results from a non-invasive treatment with no recovery time, no scar, and no permanent numbness in the toes is a meaningful number. The authors concluded that focused shockwave can be considered as a treatment option before minimally invasive and surgical techniques.
So the honest summary is this. Surgery still produces the highest rate of full relief, but it is irreversible and comes with real downsides. Shockwave does not work for everyone, but it works for most people who try it, and the safety profile is excellent. A systematic review of shockwave therapy across orthopedic conditions published in the British Medical Bulletin concluded that shockwave is a safe modality when applied by trained clinicians, with a low rate of serious adverse events.
For someone trying to avoid surgery, that math is usually worth a try.
HOW DOES SHOCKWAVE THERAPY WORK ON A PINCHED NERVE IN THE FOOT?
Focused shockwave therapy uses acoustic waves, not electricity, delivered through a handheld applicator. The waves transfer mechanical energy through the skin into the tissue between the metatarsal bones, exactly where the irritated nerve sits. That energy does a few things at once.
It increases blood flow in the area, which gives the local tissue more of what it needs to repair. It nudges a stalled, chronic state of low-grade inflammation back into an active healing response. And there is direct evidence that shockwave can act on the nerves themselves. A 2020 study in Advances in Clinical and Experimental Medicine showed that shockwave therapy enhanced peripheral nerve remyelination, the regrowth of the protective sheath around a nerve, in a crush injury model. That is consistent with what the clinical trials show in Morton's neuroma, where the imaging does not change much but the pain and the function clearly do.
There is also an analgesic effect that often shows up early. Shockwave appears to influence how nerve endings transmit pain signals, which is part of why people frequently notice a calming of symptoms within the first one or two sessions, before any meaningful tissue change could have happened. The bigger structural shifts take longer.

WHAT DOES SHOCKWAVE THERAPY FOR MORTON'S NEUROMA LOOK LIKE AT UNPAIN CLINIC EDMONTON?
A typical first visit is a 60-minute one-on-one assessment. Before we do anything, we confirm that what is going on actually is Morton's neuroma. The ball of the foot can hurt for several different reasons, including metatarsalgia, stress reactions in the metatarsal bones, capsulitis at one of the metatarsal joints, and forefoot tendon issues. A neuroma usually has a specific story (pebble-in-shoe sensation, burning between two specific toes, pain that worsens with tight shoes and improves the moment you take them off), and there are physical tests that help confirm it.
We also look further up. Ankle stiffness, calf tightness, weak hip muscles, and certain walking patterns all force the forefoot to take more load than it should. If we treat the foot without addressing those, the nerve keeps getting irritated even after the tissue starts to heal. So the plan usually has more than one piece.
The main piece is focused shockwave applied between the metatarsals where the nerve sits. Sessions are short, usually about 15 to 20 minutes. You feel a strong tapping sensation that we adjust to your tolerance. There is no needle and no recovery downtime. Most plans run three to six weekly visits. After most sessions, the foot feels slightly tender or warm for a few hours, which is part of the healing response.
When the area is broadly irritated, we sometimes add EMTT in the same visit. EMTT uses pulsed electromagnetic fields delivered through a loop applicator placed over the forefoot. You feel nothing during the session, just a faint clicking sound from the device. It is not used on every case, but for foot pain that involves a wider region than just the neuroma itself, it pairs well with shockwave.
Hands-on work matters too. Gentle mobilization of the small joints in the forefoot can take a bit of pressure off the nerve. Soft tissue release of the calf and the bottom of the foot reduces the load that gets transmitted up to the metatarsal heads. A short, specific exercise program at home builds the muscles that support the arch and gives the forefoot some help carrying load.
We also spend a few minutes on shoes. The right footwear during your recovery makes a noticeable difference. Wider toe box, lower heel, a slight rocker, and a metatarsal pad placed correctly behind the painful spot all help. You can keep your dress shoes for special occasions, but day-to-day, your foot needs room to breathe.
If you want to understand the technology behind shockwave in more depth, our article on how focused shockwave therapy works walks through the mechanics.

“2 years agoI have had many treatments with Uran for at least 10 years. I have had a lot of sports injuries and he has treated them all! Shockwave has helped me recover. He is so knowledgeable and I trust him always. Wouldn’t go anywhere else! Staff are amazing too. Thank-you!”- Kim Murrell
WHAT CAN I DO AT HOME TO MANAGE MORTON'S NEUROMA?
What you do between sessions matters. Five habits make a real difference. None of them is a cure on its own.
- Change your shoes. The most useful single thing you can do is move to footwear with a wide toe box, a low heel, and a slightly stiffer sole. If the front of your foot feels squeezed when you walk in your current shoes, those shoes are part of the problem. Save the narrow and high-heeled ones for short events.
- Use a metatarsal pad placed correctly. The pad goes just behind the painful spot, not directly on top of it. Done right, it lifts and separates the metatarsal heads slightly, giving the nerve more room. Done wrong, it sits under the neuroma and makes things worse. Ask us at your assessment if you are not sure.
- Cut back on the activities that flare you, do not stop moving. Long days on hard floors, running on pavement, repetitive jumping, and racquet sports often need to come down in volume while you settle the nerve. Cycling, swimming, the elliptical, and shorter walks in supportive shoes are usually fine.
- Stretch your calves. A tight calf forces more load through the front of the foot at every step. A simple calf stretch against a wall, held for 30 seconds, three or four times a day, both straight-knee and bent-knee versions, takes load off the forefoot over time.
- Ice the spot after long days. Rolling the forefoot over a frozen water bottle for 5 to 10 minutes after a long day calms the nerve down. Heat is fine for stiffness but ice is usually a better fit when the nerve is hot and reactive.
If you have done all of this consistently for six to eight weeks without progress, that is the cue to get reassessed. Something in the plan is missing.
WHAT WE DO NOT OFFER
- We do not perform injections of any kind, including cortisone, alcohol sclerosing injections, or platelet-rich plasma.
- We do not prescribe oral or topical pain medications. We are physiotherapists and registered massage therapists, not physicians.
- We do not perform surgery, including neurectomy. If your Morton's neuroma has not responded to a thorough conservative plan and surgery is on the table, we will tell you and refer you to a foot and ankle surgeon for an opinion.
- We do not perform radiofrequency ablation or other nerve-destruction procedures.
- We do not promise cures. Most people who try shockwave for Morton's neuroma get meaningful relief, but not everyone does. What we offer is an honest plan, regular review, and a team that will tell you if we are not the right fit.
FREQUENTLY ASKED QUESTIONS
Does shockwave therapy hurt?
The pulses are uncomfortable on an irritated spot in the foot, and most people rate them around four or five out of ten during the session. We adjust the intensity to what you can tolerate. After the session, a few hours of mild soreness or warmth in the forefoot is normal. There is no needle, no incision, and no medication to react to.
How many sessions will I need?
A typical course is three to six weekly sessions. Some milder cases settle in three. More stubborn ones may need five or six. We reassess as we go, and we will tell you honestly if a course is not moving you in the right direction.
Will I feel relief right away?
Some people notice the symptoms calming down after the first or second session, but the bigger gains usually show up at the four-to-twelve-week mark, after the tissue has had time to respond. That timeline matches what the published trials show. Patience helps.
I have had Morton's neuroma for years. Is it too late for shockwave?
Probably not. The trials specifically enrolled people with chronic, stubborn neuromas who had already tried conservative care. A long duration is not a reason to skip the treatment. What matters more is the size of the neuroma, the state of the tissue around it, and what else is going on in the foot and chain above it.
Can shockwave help if I have already had Morton's neuroma surgery?
Sometimes, yes. Post-surgical pain in the same area is often due to a stump neuroma, where the cut end of the nerve forms a small painful bundle, or to scar tissue around the surgical site. Shockwave has been explored for both, and there is some evidence it can help. We assess the post-surgical situation specifically before recommending a course.
Should I get a cortisone injection first?
Not necessarily. A cortisone injection can give meaningful short-term relief, but it does not change the underlying nerve compression, and repeated injections come with their own downsides, including thinning of the fat pad under the ball of the foot. Many people do try cortisone first and come to shockwave when the relief stops lasting. There is no rule that you have to do it in that order.
Do I need a doctor's referral to come to Unpain Clinic?
No referral is needed. Physiotherapists and registered massage therapists in Alberta are primary contact providers, so you can book directly. Some extended health plans require a doctor's referral for reimbursement, so it is worth checking your benefits if that matters to you.
ABOUT THE AUTHOR
Written by Uran Berisha, PT, RMT, Founder of Unpain Clinic and Medical Shockwave Institute. Uran is a physiotherapist based in Edmonton, Alberta, and an International Educator in Shockwave Therapy. Medically reviewed by Uran Berisha, PT, RMT.
READY TO STOP CHASING THE PAIN AND START TREATING THE CAUSE?
If your forefoot pain has not budged with wider shoes, a metatarsal pad, and the usual rest, the next step is a 60-minute one-on-one assessment in Edmonton where we confirm what is going on, look at the whole chain, and build you a clear, written plan. No referral needed. No pressure. We will tell you honestly whether shockwave is the right call. You can book a one-on-one assessment when you are ready.
REFERENCES
The following sources are linked inline in the body above. The full citations are listed here for completeness.
- Seok H, Kim SH, Lee SY, Park SW. Extracorporeal shockwave therapy in patients with Morton's neuroma: a randomized, placebo-controlled trial. Journal of the American Podiatric Medical Association. 2016;106(2):93-99. doi:10.7547/14-131. PMID: 27031544. https://pubmed.ncbi.nlm.nih.gov/27031544/
- Fridman R, Cain JD, Weil L Jr. Extracorporeal shockwave therapy for interdigital neuroma: a randomized, placebo-controlled, double-blind trial. Journal of the American Podiatric Medical Association. 2009;99(3):191-193. doi:10.7547/0980191. PMID: 19448168. https://pubmed.ncbi.nlm.nih.gov/19448168/
- Meyer B, Moya D. Treatment of Morton's neuroma with focused shock waves: comparison between shock waves and surgery. Journal of Regenerative Science. 2022;2(2):13-16. doi:10.13107/jrs.2022.v02.i02.055 http://jrsonweb.com/treatment-of-mortons-neuroma-with-focused-shock-waves-comparison-between-shock-waves-and-surgery/
- Park HJ, Hong J, Piao Y, et al. Extracorporeal shockwave therapy enhances peripheral nerve remyelination and gait function in a crush model. Advances in Clinical and Experimental Medicine. 2020;29(7):819-824. doi:10.17219/acem/122177. PMID: 32735402. https://pubmed.ncbi.nlm.nih.gov/32735402/
- Schmitz C, Császár NB, Milz S, Schieker M, Maffulli N, Rompe JD, Furia JP. Efficacy and safety of extracorporeal shock wave therapy for orthopedic conditions: a systematic review on studies listed in the PEDro database. British Medical Bulletin. 2015;116(1):115-138. doi:10.1093/bmb/ldv047. PMID: 26585999. https://pubmed.ncbi.nlm.nih.gov/26585999/
Related Topics